How hormonal changes in perimenopause affect insulin sensitivity, metabolism, and biological aging — and what every woman over 40 needs to know


Elena Brull, FNR
Functional Nutrition Researcher & Women's Health Journalist · May 20, 2026 · 18 min read
Author's Note
Introduction
You are in your forties. Or maybe just crossing that line.
Inside, you still feel the way you always have. Curious. Capable. Alive. It feels like yesterday that you turned twenty — that version of you is not gone, she is still very much present.
And then one morning, you stand in front of the mirror. And something is different.
Not dramatically. Not in a way anyone else would notice. But you notice. The shape is slightly altered. The clothes fit differently. The belly that was never a problem — now is.
You haven't changed much. You're eating the way you always have. Maybe even better. You're moving your body. You're sleeping, more or less.
And perhaps — just perhaps — you had finally made peace with your body. Learned to stop fighting it. To live in it with a little more grace.
And then, quietly, without warning — it changed the rules.
That is the particular cruelty of this moment. It doesn't arrive when you've given up. It arrives when you thought you had figured it out.
Is this just getting older?
You've probably heard that before. From your doctor. From the internet. From well-meaning friends who are going through the same thing and have quietly decided to just accept it.
But what if the answer isn't aging?
What if it's biology— specific, identifiable, and to a meaningful degree, addressable?
How Much Weight Do Women Gain During Perimenopause —and Why?
When you hear the words perimenopause or menopause, you likely think of one thing: estrogen. Its decline. Its absence. The hot flashes, the mood shifts, the end of a cycle.
But what most women are never told is that estrogen does something far beyond regulating fertility. It directly influences the function of the pancreas — the organ responsible for producing insulin and regulating blood sugar.
And that changes everything.
Because when you understand what is happening in this phase — and when you pay attention early enough — you have a real opportunity to prevent some of its most unwelcome consequences. Not just for your health and wellbeing. But for the way you feel in your body, the way you look, and the vitality you carry into the decades ahead.
And the evidence of this shift is already written in the bodies of millions of women — in numbers that the medical community has long documented, but rarely communicated clearly enough.
Research consistently shows that women gain an averageof 2 to 2.5 kg during the menopausal transition — and for many, the accumulation begins earlier, in perimenopause, often 2 to 4 years before the final period. A 2024 prospective study tracking perimenopausal women over one year documented significant increases in body weight, fat mass, and waist-hip ratio — alongside simultaneous decreases in skeletal muscle and protein levels. The body composition was shifting. Quietly. Measurably. Before most women had a clinical reason to investigate.
A separate analysis found that up to 69% of women gain weight during the menopausal transition. Not a minority. Not an edge case. A majority.
And yet most women are told — if they receive any explanation at all — that this is simply aging.
It is not simply aging.
The fat is not distributed randomly. It migrates. Research documents a clear shift during perimenopause: fat that once accumulated on the hips and thighs begins to accumulate viscerally — around the organs, deep in the abdomen. This is not a cosmetic change. Visceral fat is metabolically active in ways that subcutaneous fat is not. It drives inflammation, disrupts hormonal signaling, and is directly associated with cardiovascular and metabolic risk.
What is happening beneath the surface — at the level of insulin and cellular metabolism — is the subject of this series.
Why Do Women Over 40 Suddenly Gain Weight, Crave Sugar, and Lose Focus?
There is a moment many women describe in their early-to-mid forties. Not a diagnosis. Not a crisis. Just a quiet, persistent feeling that their body has started operating by different rules — rules nobody gave them.
The favorite dress that no longer zips. The afternoon slump that coffee can't fix. The cravings that appear from nowhere — like a massive wave, impossible to reason with, impossible to outrun. The brain fog that rolls in by 3pm like a dark, heavy cloud, swallowing every last trace of focus and capability.
These experiences are often underrecognized clinically. Too diffuse for a single diagnosis. Too easily attributed to stress, age, sleep, or simply being a woman in midlife.
But there is a physiological thread that runs throughall of them.
It is called insulin resistance — and for many women over 40, it begins long before anyone mentions the word diabetes.
Insulin Resistance in Women Over 40: What It Is, What Causes It, and Why It's Not Your Fault Alone
Insulin resistance is not diabetes. But it would be too simple — and not entirely honest — to say it has nothing to do with our choices.
The truth is more layered than that.
Insulin resistance can be inherited. It can be the result of years of dietary habits that, particularly in Western industrialized societies, have quietly worked against metabolic health: too much sugar, too many ultra-processed foods, too little fiber, too little movement. These are not moral failures — they are the patterns of modern life, shaped by availability, culture, and decades of accumulated habit.
And when estrogen begins to fluctuate or decline, itdoes not cause insulin resistance on its own. It amplifies what was already building beneath the surface. The hormonal shift and the metabolic history meet— and the result becomes visible.
Insulin is a hormone — a messenger — produced by the pancreas. Its job is elegant in its simplicity: when you eat, blood sugarrises, and insulin is released to help your cells absorb that sugar and use it for energy. Think of insulin as a key, and your cells as doors. Normally, the key turns, the door opens, and energy flows.

Insulin resistance is what happens when the doors start sticking.
The key is still there. The pancreas is still producing it — often in greater quantities, trying harder. But the cells become less responsive. Blood sugar stays elevated a little longer. The pancreas works harder. The system compensates — until, eventually, it may no longer be able to.
That is the slow arc toward prediabetes, and ultimately, type 2 diabetes.
But here is what matters most for this conversation: that arc begins silently, often years before any lab value crosses a clinical threshold.
And it frequently begins during perimenopause.
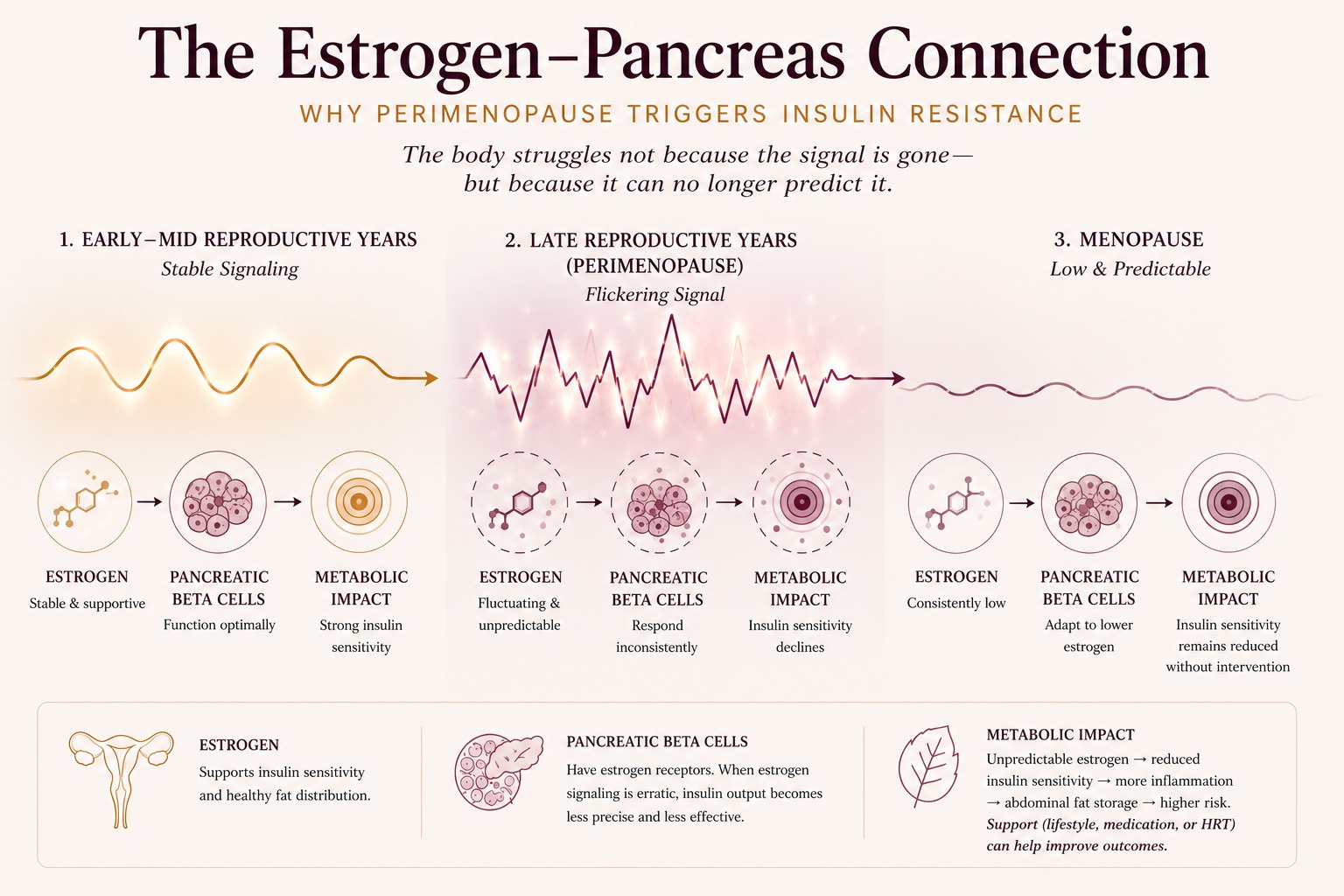
Why Perimenopause Triggers Insulin Resistance: The Estrogen-Pancreas Connection
Estrogen does far more than regulate the menstrual cycle.
Among its many roles, estrogen directly supports insulin sensitivity — the body's ability to respond efficiently to insulin's signal. It does this in part by acting on estrogen receptors in the pancreatic beta cells — the very cells responsible for producing insulin. When estrogen levels are stable, these cells function optimally. When estrogen begins to fluctuate, their output becomes less precise, less predictable, and less effective.
Estrogen also supports healthy fat distribution, favoring the hips and thighs over the abdomen — moderating inflammation and protecting the metabolic landscape in ways that only become fully apparent when it begins to waver.
And in perimenopause, it wavers — unpredictably, sometimes wildly, before it ultimately declines.
This is different from menopause, where estrogen has settled into a new, lower equilibrium. In perimenopause — the transition phase that can begin as early as the late thirties and last a decade — estrogen surges and dips without pattern. For many women, this is the most metabolically disruptive period of their lives, precisely because the hormonal signal is so erratic.
The result? Insulin sensitivity begins to shift. Subtly at first. Then with growing consequences.
The decline in insulin sensitivity during perimenopause and menopause is well-documented — and it affects far more women than current screening practices reach, including those who are slim, active,and show no obvious risk factors. A woman who appears metabolically healthy by every conventional measure may still be experiencing significant dysregulation beneath the surface — and will not routinely be screened for it. Because insulin resistance in women who don't fit the expected metabolic profile remains underdiagnosed — a silent condition in a population not yet systematically reached by standard screening.
"Perimenopause is less like a door closing and more like a room where the lights keep flickering. The body struggles not because the signal is gone — but because it can no longer predict it."
The full science of how estrogen shapes metabolism —and what happens at the cellular level when it shifts — is explored in depth in Article 2 of this series: The Science Behind the Shift — What Estrogen Does to Your Metabolism, and What Happens When It Fluctuates.
Could Your Fatigue, Cravings, and Belly Fat Be Signs of Insulin Resistance?
Insulin resistance in its early stages does not announce itself dramatically. It whispers. Through small, familiar moments that are easy to dismiss — until they aren't.
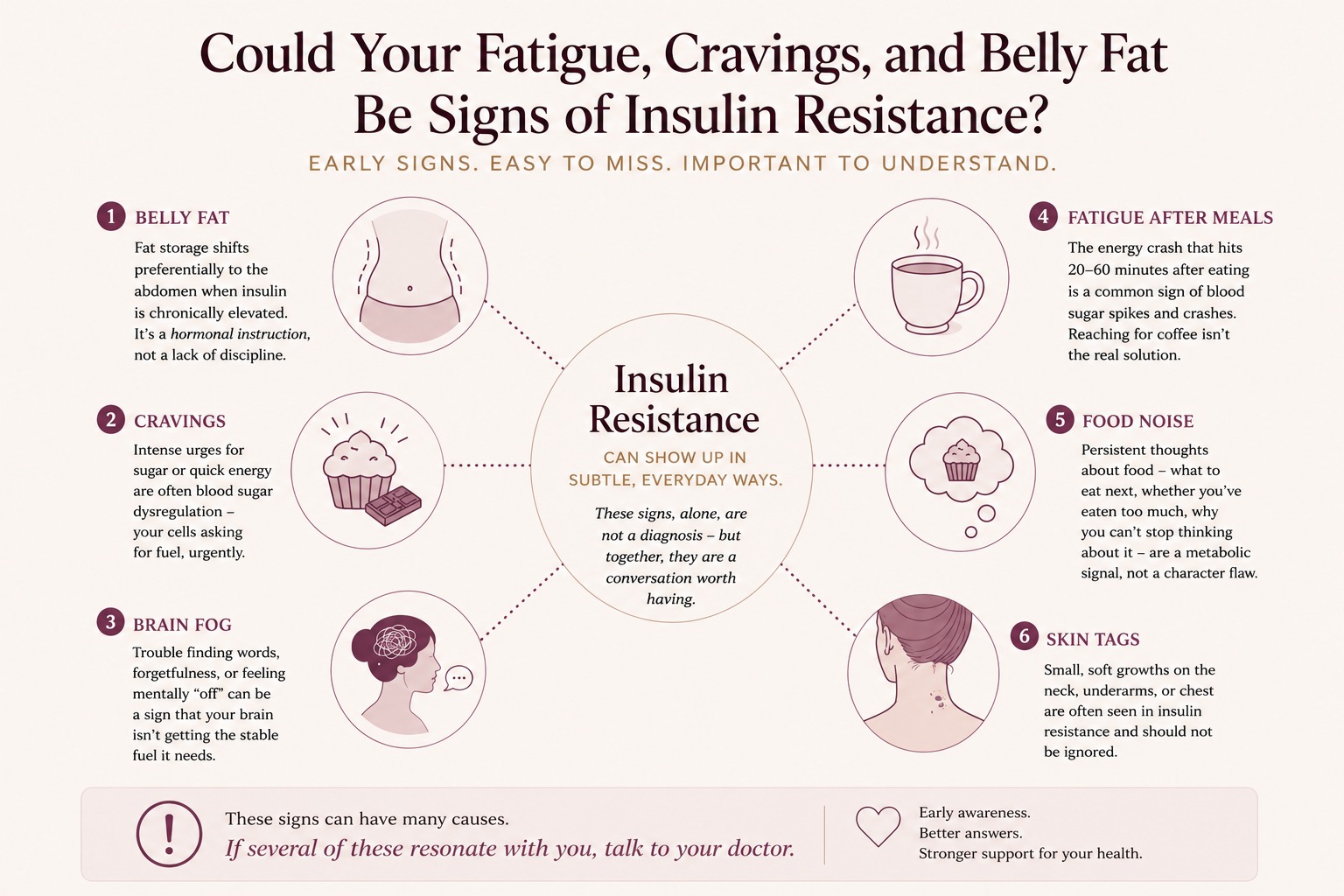
Belly fat. You open your wardrobe and find it — that little black dress that once fit so perfectly, the one that knew exactly how to flatter your figure in your twenties. You try it on. And something is off. Maybe it shrunk a little in the wash. Or maybe — and this is the thought you push away — it's the belly the dress is now quietly putting in the spotlight. That soft, stubborn roundness that wasn't there before. That no amount of effort seems to touch. When insulin is chronically elevated, fat storage shifts preferentially to the abdomen. It is not a failure of discipline. It is a hormonal instruction.
Cravings. It's 3pm. You had lunch. A proper lunch. And yet here you are, standing in front of the open fridge or the kitchen cupboard, looking for something — anything sweet, anything with a quick hit of energy — with an urgency like a wave you cannot reason with. This is not hunger. This is dysregulated blood sugar sending an emergency signal: the cells need fuel, and they need it now. A physiological demand, not a lack of willpower.
Brain fog. You are in a meeting. A colleague says something, turns to you, waits for your response. And the word you need — a word you know, a word you have used a hundred times — is simply not there. The thought dissolves before you can catch it. You smile, you navigate, you compensate. But later, alone, you wonder: what is happening tome? This is not distraction. This is the brain's access to stable,consistent fuel — disrupted.
Fatigue after meals — the energy crash thatarrives twenty minutes after eating, sending you toward the coffee machine whenwhat you really need is none of what you're craving.
Food noise — what many clinicians and patients now describe as a persistent, background mental preoccupation withfood: what to eat next, whether you've eaten too much, why you can't stop thinking about it. Many women experience this as a character flaw. It is increasingly recognized as a metabolic signal.
Skin tags — small, soft growths that appearon the neck, underarms, or chest. Often dismissed as harmless. Recognized in clinical literature as a cutaneous marker of insulin resistance.
None of these signs, alone, is a diagnosis. But together, they are a conversation worth having — with your doctor, and with yourself.
Calorie Restriction and Insulin Resistance — The Diet Trap Women Over 40 Fall Into
You are at your annual check-up. The nurse notes your weight. You glance at the number — and pause. It is not dramatically different. But it is different enough. And when you mention it to your doctor, the answer comes quickly: "That's normal for your age." You leave with no further explanation. And the reaction, when you get home, is almost universal: eat less. Move more. That seems to be the well-kept secret of every slim woman.
Or perhaps something more radical. Fasting? A juicecleanse? Keto?
And so it begins — the experimentation that so many women in their forties know intimately. The smoothie diet, the elimination diet, the intermittent fasting protocol. And at first, the weight drops. It works. It feels like control.
Until it doesn't.
Because there comes a moment — when you can no longer stand the sight of another green smoothie, when the cravings for something warm, something sweet, something real become impossible to ignore — when every woman eventually finds her way back to comfort food. And that is when the nextsurprise arrives.
The metabolism, long adapted to restriction, now treats everything above that threshold as excess. And stores it. As fat. Efficiently, and without apology.
The relationship between dieting, metabolism, and women's health is far too complex to be reduced to eat fewer calories. Insulin resistance has less to do with caloric quantity than with eating habits, lifestyle, and the quality of what we put into our bodies.
But for a woman in perimenopause dealing with early insulin resistance, calorie restriction alone is one of the most misleading strategies available. Not because effort doesn't matter. But because the underlying problem is not the quantity of food. It is the body's ability to process it.
Insulin resistance is not a calorie problem. It is a metabolic signaling problem.

And here is the crucial distinction: insulin resistance does not arise because estrogen declines. It is not caused by the hormonal shift. But it is amplified by it — because a player that once participated, however indirectly, in blood sugar regulation is no longer in the game.
That distinction matters. And it changes everything about how we approach the solution.
"Counting calories when you have insulin resistance is like rationing electricity when the wiring is faulty. The problem isn't the supply. It's the circuit."
What exactly that solution looks like — which eating patterns, lifestyle shifts, and where appropriate, medical interventions actually move the needle on insulin sensitivity — is the subject of Article 6 of this series: What You Can Do — Nutrition, Movement, Sleep, and Stress as Metabolic Medicine.
Perimenopause and Body Changes: Why This Transition Feels So Disorienting
There is something about perimenopause that has not been named clearly enough.
It is a transition. A profound biological reorganization. And unlike so many of life's transitions — which announce themselves, which give you time to prepare — this one often arrives without warning. You cannot pinpoint the exact moment it changed, because it happened somewhere beneath the surface, in the quiet language of hormones and metabolism, long before the mirror showed you.
In some ways, it is reminiscent of the passage from girlhood to womanhood — that moment when the body begins changing on its own terms, with a logic that feels foreign, sometimes alarming, and rarely fully explained. The body you have inhabited for decades suddenly feels like it is operating on a different frequency. Familiar, and yet foreign. And often, a quiet shame that nobody warned you to expect.
Who is this woman in the mirror?
That question deserves an answer that is honest, informed, and kind.
The body has not failed you. It has entered a new metabolic chapter — one that nobody handed you a guide for.
HRT, Perimenopause, and Insulin Resistance
Anyone who has ever sailed knows what gusts feel like.They arrive without warning, from an unpredictable direction, with varying force. One moment the sea is calm. The next, the sail fills violently — and just as suddenly, the wind is gone.
This is precisely what estrogen does in perimenopause.
It surges. It drops. It rises again. Not in a pattern anyone can predict or plan around. And attempting to correct this with hormone therapy at this stage is a little like trying to compensate for gusts by adjusting the sails after they've already hit — by the time you respond, the wind has already changed direction.
Menopause is different. The wind does not disappear —it settles. Steady, predictable, and low. And with a constant wind — even a gentle one — you can set your sails and navigate.
This is why hormone therapy has an established role in menopause: because the signal is stable enough to work with. In perimenopause, the hormonal environment is a different matter entirely.
Hormone therapy in perimenopause is an established clinical option — and for many women, transdermal estradiol combined with progesterone can be an appropriate and effective approach. But the erratic hormonal fluctuation of this phase makes treatment considerably more complex than in menopause, where estrogen has settled into a stable, lower baseline. In perimenopause, dosing and timing require careful individualization — because the hormonal environment is too unpredictable for standardized intervention.

If you are already in menopause and want to understand your hormone therapy options in depth, we have covered this in detail in the BeMediq Journal:
For women in perimenopause, the most powerful tools available are often not pharmaceutical — they are metabolic. Lifestyle-based. Nutritional. And in some cases, supported by newer pharmacological options that work at the level of insulin and appetite regulation.
Which is why understanding what is happening first matters so much.
"The perimenopausal window is not a problem to be corrected with a single intervention. It is a complex, dynamic transition — one that requires precision, patience, and a clinician who understands the difference."
The full picture of medical options — including GLP-1, Metformin, and hormone therapy — and how each fits into the perimenopausal and menopausal context, is explored in Article 7 of this series: The Medical Options — What Works, What Doesn't, and What to Ask Your Doctor.
Blood Sugar and Aging in Women: It's Not Age That Ages You
We have talked about insulin resistance. We have talked about weight gain, about cravings, about the metabolic disruption that perimenopause quietly sets in motion.
But there is one more consequence that is almost never mentioned — and it may be the most personal of all.
Because when insulin resistance rises and blood sugar becomes chronically elevated — even subtly — it does not only affect your weight or your energy. It affects the speed at which you age.
Here is perhaps the most important reframe in this entire article.
We tend to think of aging as something that happens to us over time — inevitable, biological, written in our genes. But the science tells a different story.
It is not age alone that ages you. Blood sugar — and the metabolic environment it creates — is one of the most well-documented drivers of biological aging. Not the only one. But one that is measurable, modifiable, and rarely discussed.
When glucose remains chronically elevated — evensubtly, even within ranges not yet flagged as diabetic — a process called glycation takes place. Glucose molecules bind to collagen and elastin, the structural proteins that keep skin firm, vessels flexible, and tissue resilient. The result is the formation of Advanced Glycation End-products — AGEs. And the name, as it turns out, is not accidental.
AGEs accumulate silently. They make collagen stifferand less organized. They accelerate the visible signs of aging — in the skin, in the vessels, in the body's ability to repair and renew itself. Research from the Leiden Longevity cohort found that people with higher blood glucose levels— still within non-diabetic ranges — were perceived as measurably older than their chronological age.
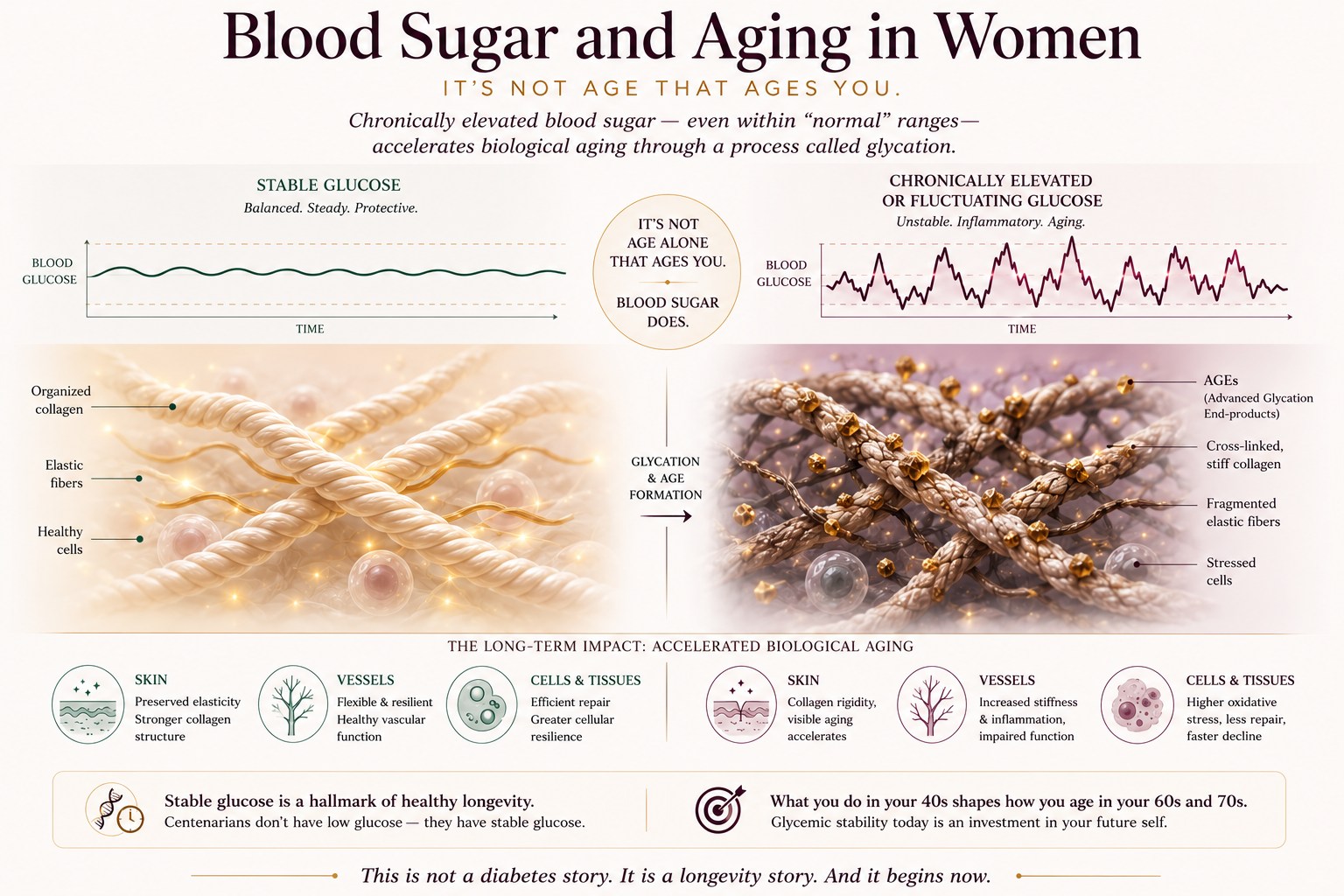
Studies of centenarians add a striking dimension: individuals who live past 100 consistently share one metabolic characteristic —not low glucose, but stable glucose. Minimal fluctuation. Sustained metabolic steadiness.
A 2022 peer-reviewed study found glucose to be among the biomarkers with the strongest correlation to biological age — with measurably accelerated biological aging documented even in pre-diabetic individuals, well before a clinical diagnosis.
And perimenopause — the precise moment when insulin resistance begins its silent rise — is the moment when glycemic stability becomes most consequential. What happens to blood sugar in your forties shapes how you look, feel, and function in your sixties and seventies.
This is not a diabetes story. It is a longevity story. And it begins now.
"It is not age alone that ages you. Blood sugar is one of the most well-documented — and most modifiable — drivers of biological aging."
The full science of how blood sugar drives biological aging — including AGEs, inflammation, collagen degradation, and what women can do about it — is explored in depth in our companion article: How Blood Sugar Accelerates Aging in Women — and What You Can Do About It. (Coming soon to BeMediq Journal.)
Early Insulin Resistance in Women: Why Acting Now Changes Everything
The silent price of ignoring early insulin resistanceis not paid today.
It accumulates. Over years. In the form of higher cardiovascular risk — because chronic insulin resistance is one of the strongest predictors of heart disease in women, a risk that rises significantly after menopause. In the form of increased inflammation, which touches nearly every system in the body. In the form of cognitive changes, because the brain relies on insulin signaling in ways science is still uncovering. In the form of the progressive narrowing of the metabolic window — the growing distance between where you are and where you want to be.
But that is not the only story.
Because early recognition changes the trajectory. Because there are interventions — nutritional, behavioral, and where appropriate, medical — that can restore sensitivity, reduce risk, and allow women to feel recognizably themselves again.
What you are experiencing has a name. And a cause. Understanding both is where the work begins.
References
- Liao S, Zhao L, Huang C, et al. One-year trajectories of nutritional status in perimenopausal women: a community-based multi-centered prospective study. BMC Public Health. 2024;24:897. doi:10.1186/s12889-024-18405-0. PMCID: PMC10976711
- Guthrie JR, Dennerstein L, Taffe JR, Lehert P, Burger HG. The menopausal transition: a 9-year prospective population-based study. The Melbourne Women's Midlife Health Project. Climacteric. 2004; 7(4):375–389. doi:10.1080/13697130400012163
- Davis SR, Castelo-Branco C, Chedraui P, et al. Understanding weight gain at menopause. Climacteric. 2012;15(5):419–429. doi:10.3109/13697137.2012.707385
- Hurtado MD, Acosta A, Shah M, et al. Weight gain in midlife women. Current Obesity Reports. 2024. PMCID: PMC11150086
- Noordam R, Gunn DA, Tomlin CC, et al. High serum glucose levels are associated with ahigher perceived age. Age (Dordr). 2013;35(1):189–195. doi:10.1007/s11357-011-9339-9.PMCID: PMC3543736
- Liao S, et al. Effects ofVariability in Glycemic Indices on Longevity in Chinese Centenarians. Frontiers in Nutrition. 2022;9:955101. doi:10.3389/fnut.2022.955101
- Uribarri J, Woodruff S, Goodman S, et al. Advanced Glycation End Products in Foods and a Practical Guide to Their Reduction in the Diet. Journal of the American Dietetic Association. 2010;110(6):911–916. PMCID: PMC3257625
- Papachristoforou E, et al. Advanced glycation end-product intake predicts insulin resistance in a sex-dependent fashion. European Journal of Nutrition. 2025. PMCID: PMC12014793
- Wang CM, et al. The effects of advanced glycation end-products on skin and potential anti-glycation strategies. Experimental Dermatology. 2024. doi:10.1111/exd.15065
- Cefalu WT, et al. Targeting glucose metabolism for healthy aging. Journals of Gerontology. 2017. PMCID: PMC5166514
- Mirzaei K, Hossein-Nezhad A, Karimi M, et al. The Association Between Dietary Patterns and Insulin Resistance: A Systematic Review. Archives of Iranian Medicine. 2016. ResearchGate
- Imamura F, O'Connor L, Ye Z, et al. Dietary patterns,insulin resistance, and incidence of type 2 diabetes in the Whitehall II Study. Diabetes Care. 2008;31(10):2049–2054. PMCID: PMC2453656
- Gojda J, Patková J, Jacek M, et al. Effect of diet composition on insulin sensitivity in humans. Nutrition, Metabolism and Cardiovascular Diseases. 2019. doi:10.1016/j.numecd.2019.05.010
- Mofrad MD, et al. Impact of Diet Composition on Insulin Resistance. Nutrients. 2022. PMCID: PMC9505491
- Mauvais-Jarvis F. Sex differences inenergy metabolism: natural selection, mechanisms and consequences. Nature Reviews Endocrinology. 2024; 20(1):15–29. doi:10.1038/s41574-023-00911-z
- Kodoth V, Scaccia S, Aggarwal B. Adverse Changes in Body Composition During the Menopausal Transition and Relation to Cardiovascular Risk: A Contemporary Review. Women's Health Reports. 2022;3(1):573–581. doi:10.1089/whr.2021.0148. PMCID: PMC9397554
- Davis SR, Lambrinoudaki I, Lumsden M, et al. Menopause. Nature Reviews Disease Primers. 2015;1:15004. doi:10.1038/nrdp.2015.4
- Carr MC. The Emergence of the Metabolic Syndrome with Menopause. Journal of Clinical Endocrinology & Metabolism. 2003;88(6):2404–2411. doi:10.1210/jc.2003-030242
- Appelman Y, van Rijn BB, Ten Haaf ME, Boersma E, Peters SAE. Sex differences in cardiovascular risk factors and disease prevention. Atherosclerosis. 2015;241(1):211–218. doi:10.1016/j.atherosclerosis.2015.01.027
- Cersosimo E, DeFronzo RA. Insulin resistance and endothelial dysfunction: the road map to cardiovascular diseases. Diabetes / Metabolism Research and Reviews. 2006;22(6):423–436. doi:10.1002/dmrr.634
- Schmitz KH, Bhatt DL, Garrard L, et al. Skin tags as a marker of insulin resistance in a multi-racial community sample. Annals of Epidemiology. 2001;11(8):557.
- Tahrani AA, Bailey CJ, Del Prato S, Barnett AH. Management of type 2 diabetes: new and future developments in treatment. The Lancet. 2011;378(9786):182–197. doi:10.1016/S0140-6736(11)60207-9
- Poganik JR, et al. Biological age is increased by stress and restored upon recovery — and glucose emerges as a leading biomarker of biological age acceleration, with measurably elevated biological age in pre-diabetic individuals. Cell Metabolism. 2023;35:807–820. doi:10.1016/j.cmet.2023.03.002
Disclaimer: These statements are for informational purposes only and have not been evaluated by the Food and Drug Administration. This content is not intended to diagnose,treat, cure, or prevent any disease. Always consult a licensed healthcare provider before starting any supplement or therapy.
About this article: This is an evidence-informed educational piece. It draws on peer-reviewed research to explain complex physiology in accessible language, but it is not itself a peer-reviewed scientific paper.

Written by Elena Brull, FNR, Functional Nutrition Researcher & Women’s Health Journalist
About the Author
Elena Brull, FNR, is a Functional Nutrition Researcher and Women’s Health Journalist specializing in integrative approaches to hormonal balance, nutrition, and longevity. Her work combines evidence-based insights with holistic health principles to help women understand their biology and live in rhythm with it. She writes from a non-clinical, educational perspective — with the intention to inform and empower, not to diagnose or prescribe.
Citation:
Brull, Elena. Perimenopause and Insulin Resistance: The Metabolic Shift Most Women Are Never Told About. BeMediq Journal, 2026. Available at: https://www.bemediq.com/blogs/insulin-resistance-perimenopause
-
-
-
Discover Products to Support Your Health & Well-Being



MIC+B12 Injection

GLP-1 Weight Loss Program

Science Spotlight
Curious About the Science behind this Article?
Similar articles for You
























All diagnoses, treatment decisions, and prescriptions are made solely by licensed healthcare professionals after reviewing each patient’s health information. Payment does not guarantee a prescription, medication, or specific outcome.
Medication images and product visuals shown on this website are for illustrative purposes only. Actual formulations, packaging, and labeling may vary. Some medications available through BeMediq™ may be custom-compounded by licensed 503A U.S. pharmacies. These compounded formulations are prepared for individual prescriptions, have not been reviewed or approved by the U.S. Food and Drug Administration (FDA), and may differ from FDA-approved products. However, ingredients are typically sourced from FDA-registered suppliers, and pharmacies operate in compliance with state and federal compounding regulations.
Statements about potential benefits have not been evaluated by the FDA. These products are not intended to diagnose, treat, cure, or prevent any disease. Individual results may vary. Medications should only be used as directed and under the supervision of a licensed provider.
BeMediq™ is not affiliated with, endorsed by, or sponsored by the manufacturers of FDA-approved brand-name drugs such as Ozempic®, Wegovy®, Mounjaro®, or Zepbound®. These trademarks are the property of their respective owners.BeMediq™ services are intended for adults 18+ and are not for use in emergencies. If you are experiencing a medical emergency, call 911 or seek immediate in-person care. Availability of services may vary by state and is subject to provider licensure and applicable regulations.
All health data is handled securely in accordance with HIPAA and applicable privacy laws. Please review our Terms of Service and Privacy Policy for more information.
